The YIMBY-Libertarian Convergence
A eminent domain case out of Rhode Island shows how YIMBY regulatory reforms and libertarian constitutional law activism work in tandem.
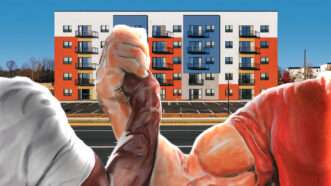
A eminent domain case out of Rhode Island shows how YIMBY regulatory reforms and libertarian constitutional law activism work in tandem.

Plus: FIFA’s president doesn’t understand his own organization's politics; a solid new pickleball movie

Plus: Surveillance for babies, using endowments to keep lights on, and more...

The liberal justice wants the Supreme Court’s harshest progressive critics to chill out.


Plus: Trump restarts talks with Iran, the Warner Bros.-Paramount merger, and Congress revisits the COVID response.

Trump opposes foreign influence in American politics, but his State Department is offering millions of dollars to promote Western identity and opposition to “mass migration” abroad.

The ban on new foreign-made robotic devices comes soon after regulators nearly killed Roomba maker, iRobot.

An invented name, recycled evidence, and an openly lawless proceeding kept prisoners guessing. The clearest signs of release were extra food, sunlight, and medical attention.

The acting attorney general confirms his dishonesty in presenting that jaw-dropping scam as the resolution of a bona fide legal dispute.

We’re locked in a cycle: The president threatens to resume the war, he claims Iran backed down, and then he gets frustrated with Iran again.

"He should never have been charged, let alone convicted," judges now say.
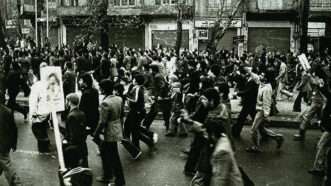
A regretful rebel talks about what he learned from his participation in Iran’s Islamic revolution.
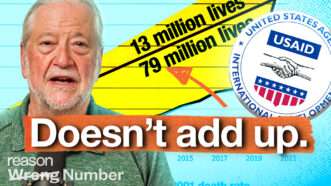
The study cited by Rep. Ro Khanna as the basis for that claim is statistical nonsense.

It's been more than eight years since Trump's first aluminum tariffs were imposed. How long do we have to wait before calling this a failure?


The judge concluded that a high school student's privacy interests trumped freedom of the press.

The New York City mayor painted a target on wealthy taxpayers.

By lifting the hold on foreign physicians, the Trump administration tacitly admitted its broad immigration restrictions aren't working.


A new collection of Whitman's writing is a fitting read for the United States' 250th birthday.

The president is still pushing the idea of using taxpayer money to reward Capitol rioters, contradicting the attorney general nominee's assurance that it won't happen.

Michael Soyfer, an attorney at the Institute for Justice, calls it “just the tip of the iceberg.”

Casting Kalshi as an out-of-control gambling platform makes it easier for the state to take money from the company and its users.

Paul Skalnik was a career criminal and jailhouse snitch whose unbelievable testimony secured dozens of convictions—including that of Jim Dailey, who awaits execution.

The Kansas Justice Institute argues that Wichita's "warrantless ALPR dragnet surveillance program" violates the state constitution's privacy protections.

Venezuela’s government-run grocery stores led to endless lines, empty shelves, quotas, and corruption.

The Expedited Access to Biosimilars Act enables FDA approval of pharmaceutically equivalent biologic medications.

Zoox got the first commercial exemption for a driverless car. It came with a promise that safety regulations would evolve “as Zoox's technology advances.”

"There is no domestic alternative" for peppercorns grown in Zanzibar or herbs from the south of France, says Ori Zohar, the former Shark Tank contestant taking the administration to court.

A darker, more adult Spider-Man movie that works best when it's just about Spider-Man.

Plus: Baby bust affects college enrollment, migrants flood into Spain, I'm writing a book, and more...

Apple TV's new horror comedy shows us that succubi and killer clowns are the real result of politicians doing evil in the name of the greater good.


Constitutional limits on federal authority should not be partisan matters.

The president’s protectionism has constituted the largest tax increase since 1993.
Transaction Denied explains how the feds pressure banks to punish disfavored groups like the NRA.

The ACLU of Iowa found that black and disabled students were disproportionately the subject of police referrals and arrests for school disciplinary issues.

Will they be held responsible for the illegal search and the damage to his property?
Robby Soave and Christian Britschgi argue that Anthony Fauci has never fully accounted for the damage caused by COVID lockdowns—and they are not ready to forgive him for it.


A new bipartisan bill would ban manufacturers from selling cars in the U.S. if more than 15 percent of shares are Chinese-owned.

Researchers estimate that discouraging just one-third of international STEM graduates could leave the American economy 0.7 percent to 1.3 percent smaller—equivalent to losing the entire economy of Utah or South Carolina.

By haggling over the details of Trump's flagrantly corrupt IRS "settlement," dissenting Republican senators give a pass to Blanche's unethical and illegal approval of it.

The 30-year U.S. Treasury bond just hit its highest yield level since 2007.

As U.S. attorney, Jay Clayton subpoenaed journalists for reporting embarrassing information about the president's new plane.
Celebrate your independence with a subscription to Reason magazine, your most trusted source of honest, insightful news and analysis.




