Alarm About a 'Heroin Epidemic' Skyrockets As Heroin Use Falls
Yesterday the Substance Abuse and Mental Health Services Administration (SAMHSA) released the results of the 2013 National Survey on Drug Use and Health (NSDUH). As I noted a couple of weeks ago, when SAMHSA gave us a preview of those data, the number of respondents who reported using heroin in the previous month fell by 14 percent last year, despite ever-rising concern about a new "heroin epidemic." While NSDUH probably misses a substantial number of heavy users (exactly how many is unclear), the trends identified by the survey still should indicate whether heroin consumption is on the rise or on the wane (as both government officials and journalists tend to assume). Hence it is instructive to compare past-month heroin use measured by NSDUH (in thousands of users) with mentions of a "heroin epidemic" in the newspaper and wire service articles collected by Nexis:
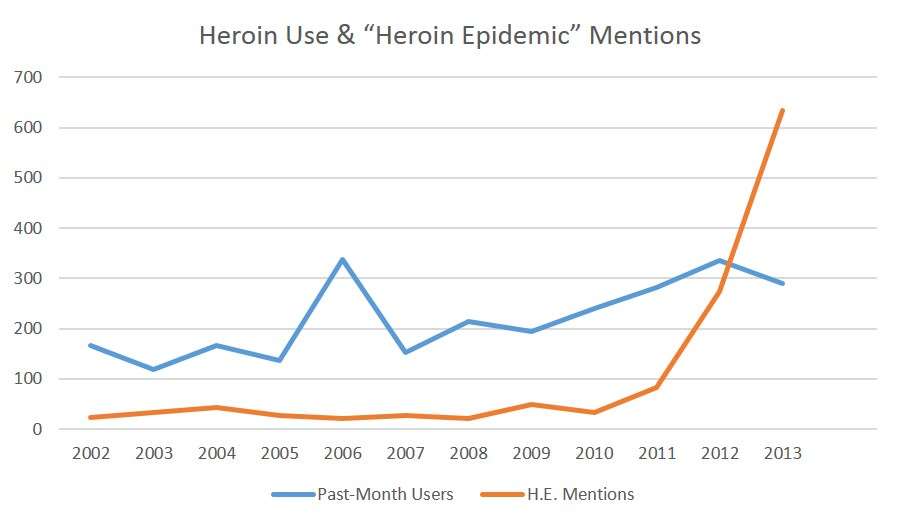
On the face of it, there is no obvious relationship between the level of heroin use and the level of press attention to it. Notice that the spike in 2006, when the number of past-month users was higher than it has been in any year since then, seems to have prompted no journalistic response whatsoever. The more gradual increase seen after 2009, by comparison, coincided with an initial drop in "heroin epidemic" mentions, followed by a slight increase. Then the number of mentions skyrocketed, rising from 82 in 2011 to 273 in 2012 and 633 in 2013. So far this year there have been nearly 2,300 references to a "heroin epidemic" in these news sources, reflecting the tremendous attention attracted by the actor Philip Seymour Hoffman's death on February 2 (which was caused by "mixed drug intoxication" but generally attributed to heroin alone). That single incident seems to have generated more talk of a "heroin epidemic" than everything else that happened in the previous 12 years. In any case, coverage of the putative epidemic really took off around the time when heroin use started to fall.
This disconnect between drug use and public alarm about it is a pretty familiar phenomenon by now. Ronald Reagan ramped up the war on drugs at a time when drug use was already declining. His successor, George H.W. Bush, gave his "bag of crack" speech years after cocaine consumption peaked (as measured by NSDUH's predecessor, the National Household Survey on Drug Abuse). Just as Hoffman's death seems to be the single most important factor driving the recent explosion in press coverage of heroin, the 1986 death of basketball player Len Bias, at a time when cocaine use was falling, drove the political panic that gave us insanely disproportionate federal crack sentences (even though Bias snorted cocaine rather than smoking it).
As the sociologist Nicholas Parsons points out in his recent book Meth Mania, press panics about speed likewise have been only tenuously related to the number of people consuming it. Parsons found that coverage of methamphetamine in Time and The New York Times shot up in 1967, driven largely by a single incident: the rape and murder of Linda Fitzpatrick, the 18-year-old daughter of a wealthy Greenwich, Connecticut, couple who dropped out of an exclusive private school and reportedly got hooked on Mephedrine. In that respect, Linda Fitzpatrick was the Philip Seymour Hoffman (or Len Bias) of her day.




