As More Death Data Becomes Available, COVID-19 Looks Less and Less Like the Flu
Death data from New York State demonstrates a stark difference between the two contagious viruses

Flu versus COVID-19? Which is worse? It is quite true that the Centers for Disease Control and Prevention (CDC) data on recent flu deaths report that the number of deaths attributed to coronavirus infections has not yet exceeded estimates for the annual death tolls for the last nine influenza seasons, except for the mild outbreak in 2011-2012. However, keep in mind that the flu season generally runs from October to April, whereas person-to-person community spread of the novel coronavirus was first recognized at the end of February in Washington state.
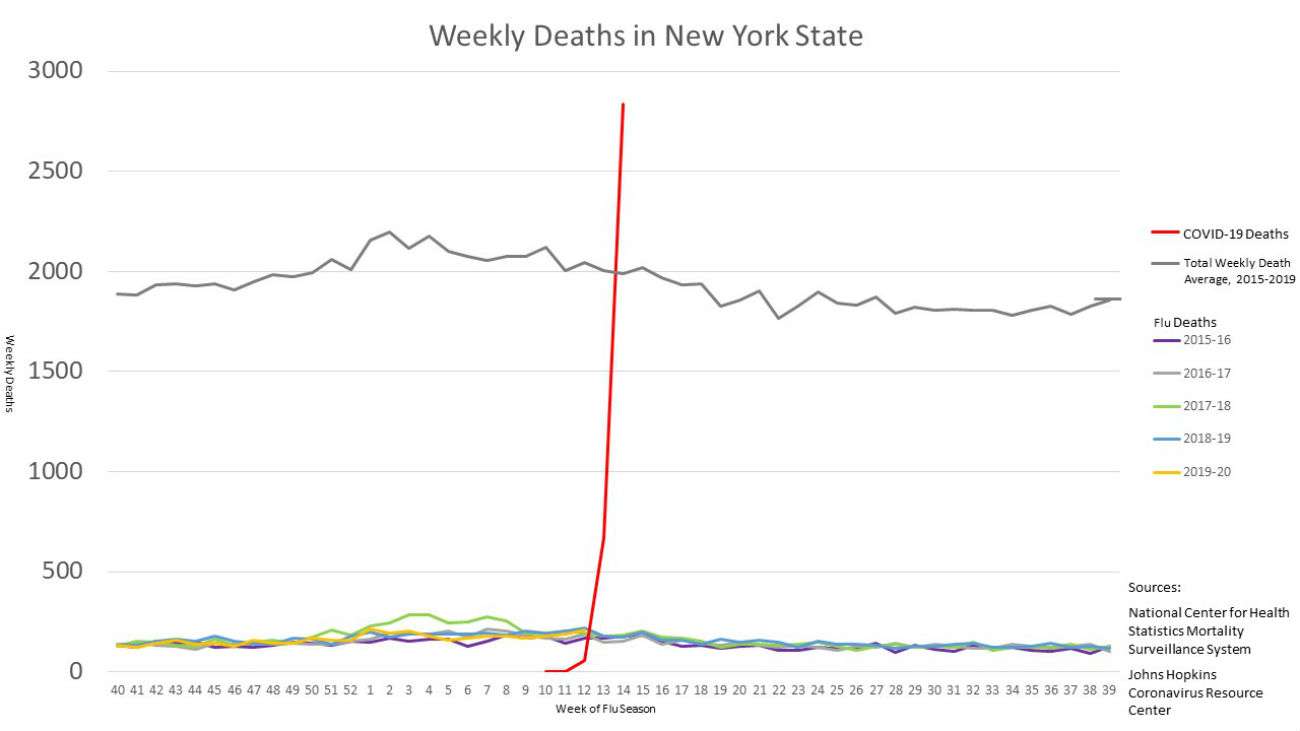
To get a better handle on the differences between seasonal flu and COVID-19, Max Roser and his team over at the invaluable OurWorldInData compared the average number of weekly deaths in New York State from influenza and all other causes versus the weekly number of deaths from the current COVID-19 outbreak. Keep in mind that the first New York COVID-19 death was reported just four weeks ago. The comparison is worrisome.
The good news is that the COVID-19 epidemic in New York may be nearing its peak.




