The Volokh Conspiracy
Mostly law professors | Sometimes contrarian | Often libertarian | Always independent
N.Y. Rationing COVID Drugs Based on Race
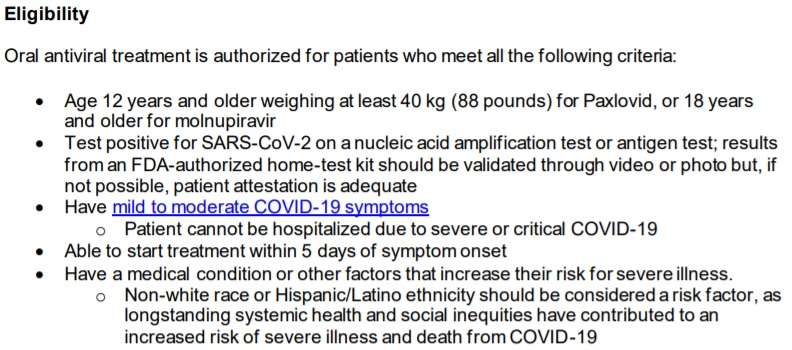
Sick non-Hispanic whites can only get oral antivirals if they have a medical condition or unspecified "other factors that increase their risk for severe illness"; sick "[n]on-white[s]" and "Hispanic[s]" don't face such a requirement.
That's from the N.Y. State Department of Health, Dec. 27, 2021. The full list:
As Glenn Greenwald points out:
That means that a healthy twenty-year-old Asian football player or a 17-year-old African-American marathon runner from a wealthy family will be automatically deemed at heightened risk to develop serious COVID illness—making them instantly eligible for monoclonal treatments upon testing positive and showing symptoms—while a White person of exactly the same age and health condition from an impoverished background would not be automatically eligible.
This policy was first flagged by New York journalist Karol Markowicz, whose Twitter summary described it as "white people need not apply." That summary is not accurate. White people who are sick from COVID can still be eligible for antibody treatment, but only if they first demonstrate that they have "a medical condition that increase[s] their risk for severe illness." But non-white people have the significant advantage of being automatically eligible without having to demonstrate that, since their non-white race is deemed to inherently constitute an increased risk of severe illness or death from COVID-19. In other words, when determining eligibility for life-saving treatments, New York state is explicitly prioritizing some races over others.
For more of Greenwald's detailed analysis, see here. Thanks to Hans Bader (Liberty Unyielding) for the pointer; as he points out, such use of race as a proxy for supposed greater risk—instead of focusing on the more directly relevant factors ("race-neutral alternatives," in doctrinal terms), such as underlying medical conditions, vaccination status, lack of access to good alternative care, or the like—would violate the Equal Protection Clause in this situation.
UPDATE: My UCLA colleague Prof. John Villasenor points out this provision of the New York Constitution:
§11. No person shall be denied the equal protection of the laws of this state or any subdivision thereof. No person shall, because of race, color, creed or religion, be subjected to any discrimination in his or her civil rights by any other person or by any firm, corporation, or institution, or by the state or any agency or subdivision of the state.




