The Volokh Conspiracy
Mostly law professors | Sometimes contrarian | Often libertarian | Always independent
Coronavirus Deaths Return to March/April Levels in Europe, U.S.
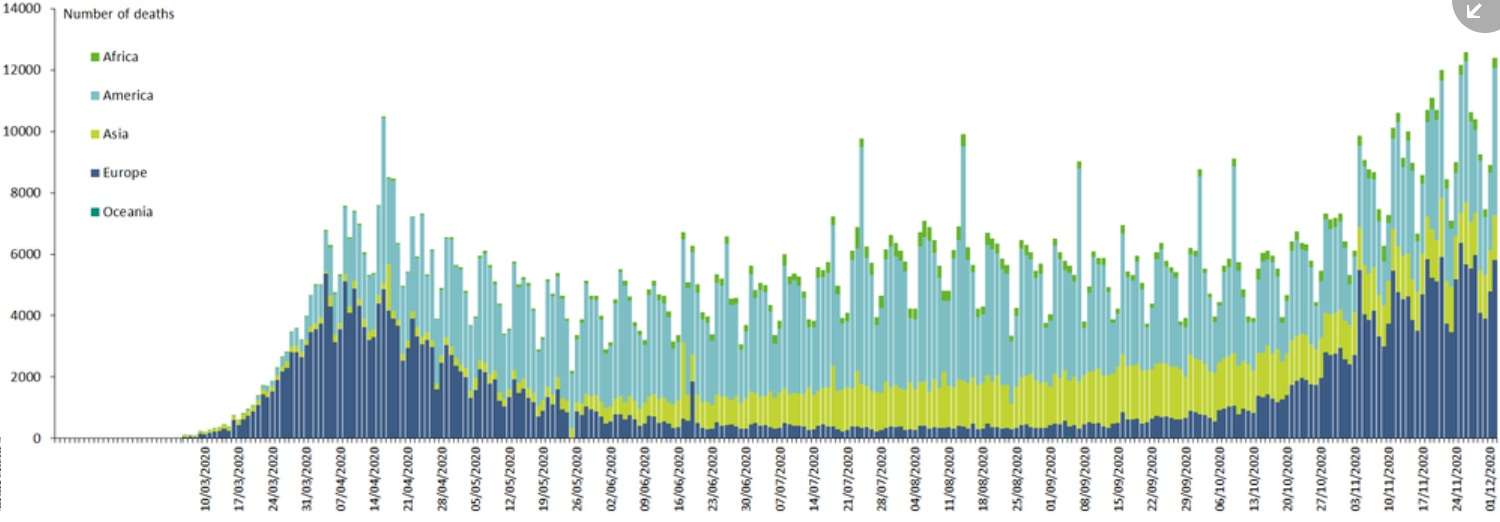
Here is the data from the Europe Center for Disease Prevention and Control; the blue bars are the totals for Europe (note that the dates are in the European format, DD/MM/YYYY):
And here is the data from Worldometers site for the U.S.:
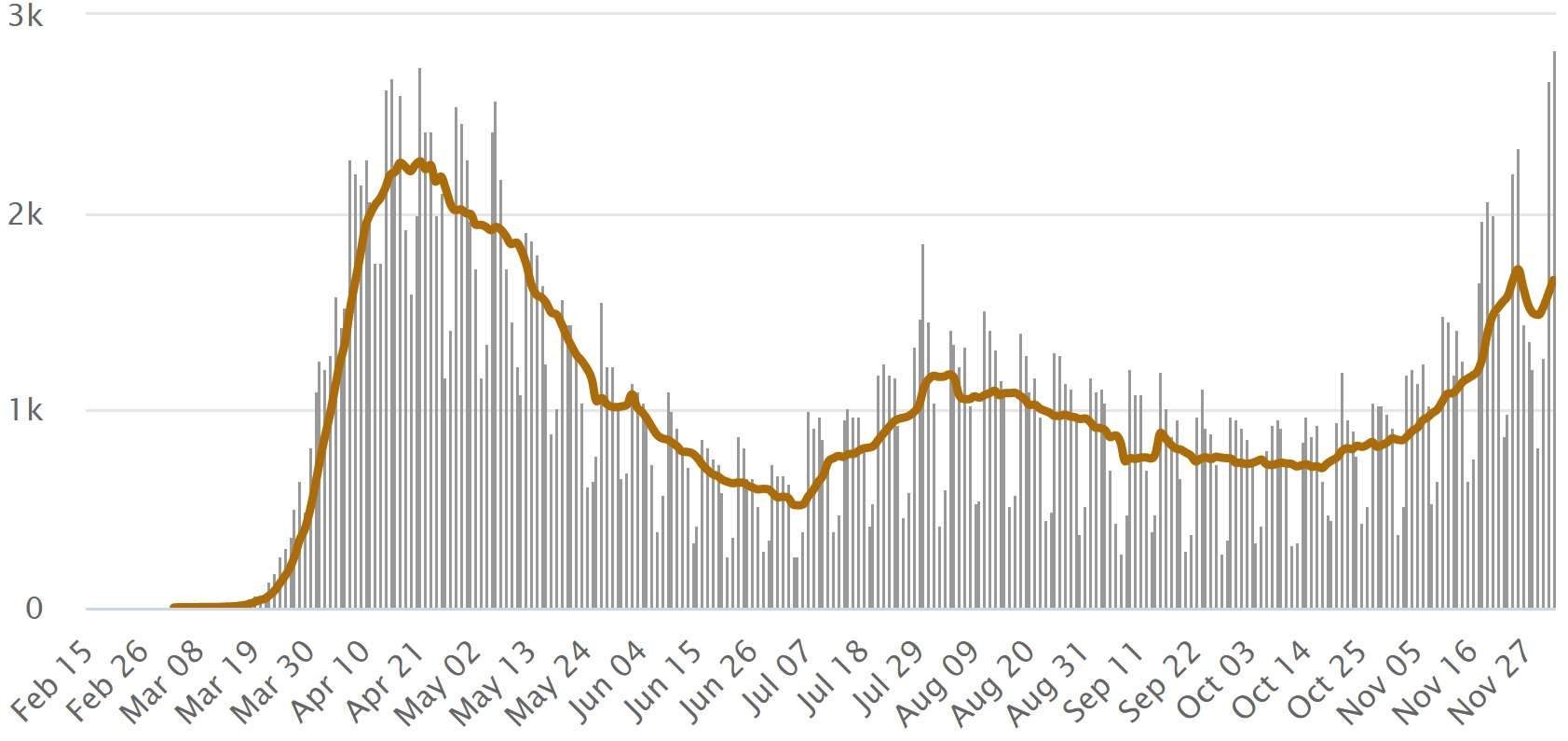
As you can see, the U.S. daily numbers (the grey bars) are comparable to the April peak, though the 7-day rolling average (the brown line) isn't yet up there. The per capita numbers in Europe (which has a population of about 2.25 times the U.S.'s) are a bit higher than in the U.S., though over the Summer they were much lower. Let's hope those vaccines we're hearing about are coming soon ….