How To Reverse an Opioid Overdose
(sun147/Fiverr)
The overdose-reversal drug naloxone is available without a prescription at most CVS and Walgreens pharmacies. It's legal to carry it, and having some on hand could help you save a life.
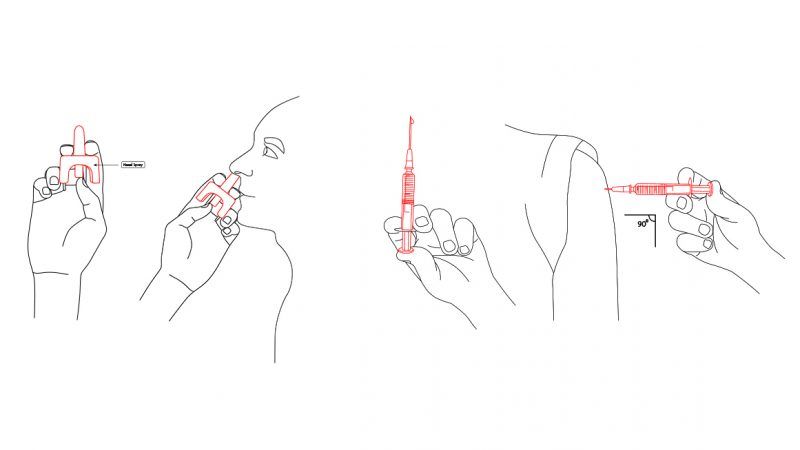
Naloxone comes in two formulations: an intramuscular injector and a nasal spray. That means reversing an overdose is as simple as jabbing a needle into someone's arm, thigh, or buttocks or squirting the drug up the person's nose.
Signs of an overdose include nonresponsiveness, cold and clammy skin, and shallow or stopped breathing.




