National Study Debunks Helena Smoking Ban Miracle (Again)
An analysis of data from nearly 2,000 counties finds no evidence that smoking restrictions produce short-term reductions in heart attacks.

If the people who promote the idea that smoking bans immediately slash heart attacks were interested in the truth, as opposed to another argument for a policy they already support, a study published this month in the journal Medical Care Research and Review would make them retract that outlandish, biologically implausible claim. Looking at county-level data from 28 states, the study finds "smoking bans were not associated with acute myocardial infarction or heart failure hospitalizations."
That will come as a surprise to anyone who accepted the propaganda peddled by anti-smoking activists at face value. Since 2003, when supporters of a smoking ban in Helena, Montana, announced that the ordinance had miraculously cut heart attacks in half during the first six months it was in effect, such claims have become conventional wisdom within the tobacco control movement. They were even endorsed by the Institute of Medicine, a division of the National Academy of Sciences, in an embarrassing 2009 report that disregarded obvious methodological problems and replaced science with wishful thinking.
As Rice University health economist Vivian Ho and the other authors of the new study point out, "Each of the studies the Institute of Medicine reviewed had at least one important limitation, such as a small study population, lack of a contemporaneous control population, or failure to account for the full range of factors that could influence hospitalizations for smoking-related conditions, such as increased cigarette taxes and local patient and health care market characteristics." Ho et al., by contrast, studied 390 counties that adopted "comprehensive public place smoking bans" from 2001 through 2008, along with 1,511 counties that did not. They controlled for potential confounding variables such as cigarette tax rates and local demographics, and they took into account pre-existing local trends.
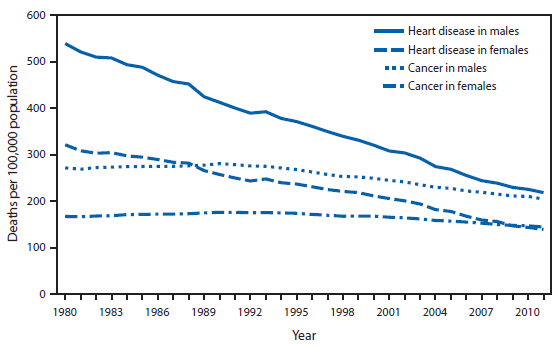
Heart disease death rates have been declining for decades in the United States, so a drop in the hospitalization rate for acute myocardial infarction (AMI) after the implementation of a smoking ban could be due to that nationwide trend rather than any local development. Furthermore, thousands of jurisdictions around the world have adopted smoking bans, and some of them were bound to see above-average reductions in AMI admissions afterward purely by chance. Focusing just on those places, as anti-smoking activists tend to do, creates a misleading impression. And even if it turned out that jurisdictions with smoking bans tended to see bigger reductions in AMI hospitalization rates than other jurisdictions, that difference could be caused by factors other than the ordinances. Ho et al. found, for example, that jurisdictions adopting bans during the study period tended to tax cigarettes more heavily in 2001 and impose larger tax hikes by 2008.
"In adjusted analyses that accounted for cigarette tax rates and population and health care market characteristics," the researchers report, "comprehensive public place smoking bans were not associated with lower AMI or heart failure hospitalization rates." As they note, that result is consistent with the findings of another national study, published by the Journal of Policy Analysis and Management in 2010, in which Kanaka Shetty and his colleagues at the RAND Corporation found "smoking bans are not associated with statistically significant short-term declines in mortality or hospital admissions for myocardial infarction or other diseases." Although those data were available in a working paper when the Institute of Medicine studied the issue, they were conveniently omitted from its report. Ho et al. say their study, while reaching essentialy the same conclusion as Shetty et al., is stronger because it used comprehensive hospitalization data rather than the 20 percent sample on which the earlier analysis relied.
"Contrary to most previous studies, we found no evidence that comprehensive public place smoking bans lowered hospitalization rates in the short term for AMI or heart failure," Ho et al. write. "The relative absence of studies concluding that smoking bans do not lower hospitalization rates may be due to publication bias." They note that Shetty et al. "found that large short-term increases in AMI incidence following a smoking ban are as common as the large decreases reported in the published literature." Overeager advocates of smoking bans created the illusion that such ordinances are typically followed by dramatic declines in AMI admissions by highlighting the places where that happened and ignoring the places where it didn't, including the places where admissions actually went up.
Ho et al. conclude that "public health officials must maintain a realistic perspective of the potential benefits and their timing when considering the effects of multiple policies to reduce smoking." Boston University public health professor Michael Siegel, who supports smoking bans but has often criticized allies who oversell their benefits, is less diplomatic. Promoters of the supposed Helena miracle "were able to disseminate their pre-determined conclusions widely to the public through the media long enough for the conclusions to be generally accepted," he writes. "Now, it is too late to undo the damage. The media and the public have already made up their minds, and one article noting the results of this new study is not going to correct or undo 10 years of dissemination of unsupported and errant scientific conclusions."





{kind=link}