Is Marijuana a Gateway to Opioids?
The association between cannabis consumption and use of other drugs is clear, but its meaning is not.

During a hearing on the 1937 law that effectively banned cannabis throughout the United States, a congressman asked Federal Bureau of Narcotics Commissioner Harry Anslinger "whether the marihuana addict graduates into a heroin, an opium, or cocaine user." Anslinger, who at that point was blaming marijuana for inspiring outbursts of vicious and irrational violence, said he had seen no evidence that its users progress to other drugs. "I have not heard of a case of that kind," he said. "I think it is an entirely different class. The marihuana addict does not go in that direction."
By the early 1950s, Anslinger had changed his mind. "Over 50 percent of those young [heroin] addicts started on marijuana smoking," he told a congressional committee in 1951. "They started there and graduated to heroin; they took the needle when the thrill of marijuana was gone."
Anslinger reiterated that point four years later, when he testified in favor of stricter penalties for marijuana offenses. "While we are discussing marijuana," a senator said, "the real danger there is that the use of marijuana leads many people eventually to the use of heroin." Anslinger agreed: "That is the great problem and our great concern about the use of marijuana, that eventually if used over a long period, it does lead to heroin addiction."
The idea that marijuana use "leads to" heroin use, eventually known as the "stepping-stone" or "gateway" theory, became a durable theme of anti-pot propaganda, echoes of which can still be heard today. As vice president, Joe Biden, currently the leading contender for the Democratic presidential nomination, said "I think legalization is a mistake" because "I still believe it's a gateway drug." A couple of years ago, before coming around on legalization, New York Gov. Andrew Cuomo likewise worried that "marijuana leads to other drugs, and there is a lot of proof that is true."
Was Cuomo right about that? Was Anslinger onto something when he warned that today's pot smoker is tomorrow's heroin addict?
Anslinger was right that people who use marijuana are more likely than people who don't to eventually try heroin. But the nature of the relationship between cannabis consumption and the use of "harder" drugs remains controversial: Does marijuana use cause opioid use and, if so, in what sense? Can the association be explained by factors that independently predispose people to use both kinds of drugs?
These questions take on added significance given the ongoing collapse of marijuana prohibition across the United States, a development that has coincided with a surge in opioid-related deaths. But despite the superficial appeal of linking those two trends, the evidence suggests that legalizing marijuana does not cause an increase in opioid-related harm and may in fact mitigate it.
Clear Correlations, Contested Causes
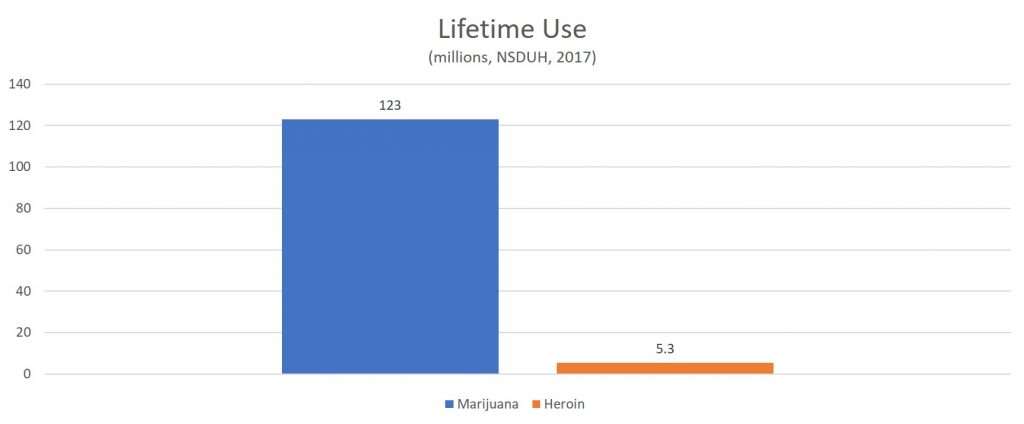
It clearly is not true that marijuana use inexorably leads to heroin use, as Anslinger sometimes implied. Recent data from the National Survey on Drug Use and Health indicate that 123 million Americans have tried marijuana, while 5.3 million have tried heroin. In other words, marijuana use is more than 20 times as common as heroin use, and less than 5 percent of cannabis consumers have tried heroin.
It is true, however, that people who use "hard drugs" such as heroin generally have used marijuana first. In a group of about 1,200 New Yorkers followed from high school into their mid-30s, for example, around 95 percent of the subjects who had used illegal drugs other than marijuana had started with cannabis.
It is also true that people who use marijuana are more likely than people who don't to subsequently use other illegal drugs. In the study of New Yorkers, men who had used marijuana by their mid-20s, but had not used it in the previous year, were almost five times as likely as men who had never used marijuana to report using other illegal drugs. The corresponding risk ratio for men who had used marijuana daily in the previous year was 12 to 1. The association between cannabis consumption and other illicit drug use is especially strong among heavy marijuana users and people who begin using marijuana at an early age.
A 2013 analysis of data from the National Survey on Drug Use and Health found that young men and women who had used marijuana were two-and-a-half times as likely to report illegal use of prescription opioids. A 2017 analysis of data from the National Epidemiologic Survey on Alcohol and Related Conditions found a similar risk ratio after adjusting for several potential confounders.
While these correlations are clear, their meaning is not. One possible explanation is that the experience of using marijuana makes people more likely to try other illegal drugs. Another possible explanation is that people who use marijuana are different from people who don't in ways that also affect their likelihood of using other drugs. Pre-existing differences in genetics, personality, and environment could explain both tendencies.
The psychologist Andrew Morral and his colleagues at the RAND Drug Policy Research Center have shown that an underlying propensity to use drugs, combined with the relative availability of different intoxicants, could entirely account for the three phenomena emphasized by advocates of the gateway theory: 1) that people tend to use marijuana before other illegal drugs, 2) that people who use marijuana are more likely to use other illegal drugs, and 3) that the likelihood of progression increases with the frequency of marijuana use. Their mathematical model did not disprove the gateway theory, but it did prove that the gateway theory is not necessary to explain these observations. Morral et al. concluded that "available evidence does not favor the marijuana gateway effect over the alternative hypothesis that marijuana and hard drug initiation are correlated because both are influenced by individuals' heterogenous liabilities to try drugs."
Twins and Rats
Several studies have sought to test the gateway theory by taking into account other variables that may be independently associated with drug use. A longitudinal study of teenagers and young adults in New Zealand, for example, found a strong association between frequency of cannabis consumption and use of other illegal drugs after adjustment for nearly three dozen potential confounding variables. But as Morral et al. pointed out, even such extensive efforts to control for confounders are unlikely to do so perfectly. They calculated that when adjustment for confounding "fails to capture just 2% of the variance in drug use propensity," marijuana users "appear to have odds of initiating hard drugs that are twice as great as non-users of marijuana." Hence "it is hardly surprising that controlling for these covariates does not eliminate the association between marijuana and hard drug use."
Another approach examines this association in twins, who share the same home environment and have similar or, in the case of monozygotic pairs, identical genes. An Australian study found that in cases where one twin had used marijuana before turning 17 and the other had not, the first twin was more than twice as likely to use opioids, regardless of whether the twins were identical or fraternal and even after adjusting for several potential confounders. A similar study based on the Vietnam Era Twin Registry found that subjects who had used marijuana before turning 18 were nearly three times as likely to use opiates as co-twins who had not. In a study of Dutch twins, the risk ratios were higher: The subjects who had used marijuana at 17 or younger were more than 16 times as likely as their co-twins to report "hard drug" use, for instance.
Even these seemingly compelling results do not rule out the possibility that pre-existing differences can account for the associations. Whatever situational factors explain why one twin uses marijuana as a minor and the other does not may also explain why one uses opioids and the other does not. "The observation that familial factors do not entirely explain the association between early cannabis use and subsequent [drug] use, while suggesting a potential causal role for cannabis use in the development of other illicit drug use, does not prove such an association," the authors of the Dutch study noted. "There may be other factors, especially aspects of the non-shared environment (e.g., peer affiliations) preceding the onset of cannabis use that might account for the observed associations."
Another kind of research used to bolster the gateway theory involves exposing laboratory animals to tetrahydrocannabinol (THC), the main psychoactive ingredient in marijuana, and observing their subsequent use of other drugs. 
Aside from the usual problems associated with extrapolating from animal behavior in the laboratory to human behavior in the real world, the relevance of the rat research is unclear. Even if early exposure to marijuana made people more likely to enjoy heroin, that would not explain their willingness to try it in the first place. To the extent that the gateway theory focuses on the transition from using cannabis to experimenting with other drugs, sensitization seems like a red herring.
What's the Matter With Japan?
Variations in drug use patterns across generations and across cultures suggest that marijuana's role as a gateway drug is a function of social norms and black-market conditions rather than the drug's inherent properties.
A 2001 analysis of data from the National Household Survey on Drug Abuse found that the likelihood of progressing to "hard" drugs such as cocaine and heroin after using marijuana rose from 9 percent among respondents born in 1940 to 39 percent among those born in the early 1960s, then fell to 24 percent among respondents born in the early 1970s and 6 percent among those born in the late 1970s. The authors concluded that "the gateway phenomenon reflects norms prevailing among youths at a specific place and time," meaning that "the linkages between stages are far from causal." It follows, they added, that "simply restricting youth's access to gateway drugs will not necessarily reduce subsequent hard drug abuse."
A 2010 study looked at data on drug use progression in 17 countries from the World Health Organization's World Mental Health Surveys. Subjects in most countries followed the pattern typically observed in the United States, starting with alcohol or tobacco and later progressing to marijuana and other illegal drugs. But the likelihood of progression from marijuana to other illegal drugs varied across countries. It was lower in the Netherlands, for example, than it was in Belgium, Spain, and the United States. Furthermore, there were striking exceptions to the usual sequence. In Japan and Nigeria, for instance, illegal drug consumers rarely tried cannabis first.
"These results suggest the 'gateway' pattern at least partially reflects unmeasured common causes rather than causal effects of specific drugs on subsequent use of others," the authors concluded. "This implies that successful efforts to prevent use of specific 'gateway' drugs may not in themselves lead to major reductions in the use of later drugs."
Marijuana prohibition might not be an effective way of reducing opioid use even if cannabis consumption is causally related to use of other illegal drugs, depending on the mechanism involved. Cannabis consumption might lead to use of other drugs, for example, by bringing people into contact with a black market where other intoxicants are also available. Violating the law to use marijuana, especially if it goes undetected by the authorities and does not result in any punishment, might reduce psychological barriers to using other illegal drugs. People who discover through personal experience that the government's warnings about the hazards of marijuana use are overblown may be more skeptical of the government's warnings about other drugs.
Since all three of these mechanisms are contingent on government policy regarding marijuana, we might expect that loosening legal restrictions on marijuana would weaken the link between cannabis consumption and use of other drugs. That may have happened in the Netherlands, which since the 1970s has tolerated the retail sale of marijuana by so-called coffeeshops, a policy justified in part by the belief that separating marijuana from other illegal drugs would make progression less likely. A 2011 study found that "cocaine and amphetamine use are below what one would predict for the Netherlands," which suggests that "separating the soft and hard drug markets possibly reduced the gateway."
Does Legalizing Marijuana Increase Opioid Use?
If there is a causal relationship between cannabis consumption and use of other drugs that is not simply an artifact of prohibition, loosening legal restrictions on marijuana should cause an increase in opioid use. Legalization can be expected to increase marijuana use by eliminating the risk of arrest, reducing the stigma associated with the drug, and making access easier (and ultimately cheaper). As cannabis consumption becomes more common, so should use of other drugs, including opioids. Yet there is not much evidence that is happening in the states that have legalized marijuana for medical or recreational use. If anything, legalizing marijuana seems to reduce opioid use.
Studies have found that medical marijuana laws are associated with reductions in high-risk opioid use, in opioid-related hospitalizations, in admissions for treatment of opioid use disorder, in the percentage of fatally injured drivers who test positive for opioids, and in opioid prescriptions for Medicare and Medicaid patients. Consistent with those results, other studies have found that patients who use medical marijuana tend to reduce their use of prescription pain relievers.
Between 1999 and 2010, a study published in 2014 found, medical marijuana laws were associated with a 25 percent reduction in opioid-related deaths. A subsequent analysis, by contrast, found that the opioid-related death rate rose faster in 20 jurisdictions that legalized medical or recreational use between 2010 and 2016 than in states that did not. But as critics pointed out, the latter analysis misclassified several states as jurisdictions where marijuana was legally available, including Oklahoma, which did not legalize medical marijuana until 2018; Florida, Ohio, and Pennsylvania, where medical marijuana programs were not operating until after 2016; and Georgia, where medical use of cannabidiol extracts (but no other cannabis product) was only notionally allowed, since there was no legal supply.
A 2018 study found that merely having a medical marijuana law was associated with lower rates of opioid-related death until 2010. After that there was no apparent benefit from medical marijuana laws per se, but states with "legally protected and operational dispensaries" continued to see reductions, suggesting that "broader access to medical marijuana facilitates substitution of marijuana for powerful and addictive opioids." A 2019 study likewise found that "states with active legal dispensaries see a drop in opioid death rates over time."
A 2017 study found that legalization of recreational marijuana in Colorado was associated with a reduction in opioid-related deaths. A study published the following year found a similar association in Washington.
These findings are not conclusive, but they do suggest that marijuana legalization so far has not contributed to the rise in opioid-related deaths. Nor is there a clear association between rising marijuana use and rising opioid use in national data. Between 2002 and 2017, according to the National Survey on Drug Use and Health, the share of Americans who reported using marijuana in the previous month rose by more than 50 percent. Nonmedical use of prescription opioids, meanwhile, was more or less flat from 2002 through 2014, and so was the prevalence of substance use disorder involving those drugs. (Subsequent numbers are not comparable because of questionnaire changes implemented in 2015.) The prevalence of past-month heroin use doubled in 2014, but it was flat from 2002 through 2013.
Persistent Skepticism
"The stepping-stone theory holds that the adolescent begins the use of illicit drugs with marihuana, and later proceeds to heroin in the search for greater thrills," the Nixon-appointed National Commission on Marihuana and Drug Abuse noted in 1972. "The opposing viewpoint holds that the large majority of marihuana users never become heroin addicts and denies the validity of a causal relationship." The commission was inclined toward the latter view, concluding that "marihuana use per se does not dictate whether other drugs will be used."
Twenty-seven years later, a report on marijuana's medical potential from the organization that later became the National Academies of Sciences, Engineering, and Medicine (NASEM) was likewise skeptical of the gateway theory. While "most users of other illicit drugs used marijuana first," the authors said, "there is no evidence that marijuana serves as a stepping stone on the basis of its particular physiological effect." Rather, "the legal status of marijuana makes it a gateway drug."
NASEM's 
Harry Anslinger clearly was wrong when he claimed that marijuana, "if used over a long period," inevitably "lead[s] to heroin addiction." Seven decades later, we recognize that marijuana users generally do not become heroin addicts. Among Americans born in 1979, for instance, the survey data indicate that 96 percent of cannabis consumers do not move on to "hard" drugs.
It remains possible that something about the experience of using marijuana makes people more inclined to try heroin or other opioids. But that theory is by no means necessary to explain patterns of drug use in the United States or other countries. And even if there is some truth to it, the implications for marijuana policy are not obvious. If "the legal status of marijuana makes it a gateway drug," as NASEM surmised in 1999, legalizing cannabis could reduce opioid use rather than increasing it. There is some evidence that is happening in the states that have decided to allow medical or recreational use.
Regardless of whether that is true, the moral case against treating marijuana use as a crime remains strong. Even if marijuana use does make subsequent abuse of opioids more likely, that would merely count as one kind of self-harm that prohibition aims to prevent. Like other forms of paternalism, marijuana prohibition interferes with the individual's sovereignty over his own body and mind. This interference is especially objectionable because the people who supposedly benefit from it—the ones who otherwise would have used cannabis, and possibly progressed to opioids—are not the people who bear the burdens of enforcement. The fear that some people whom prohibition deters from using cannabis might otherwise become heroin addicts cannot justify using force against a much larger group of people who are violating no one's rights.